
登录
洞察 - Medicine - # Rheumatoid Arthritis-Associated Interstitial Lung Disease Subtypes and Their Risk Factors
Risk Factors for Different Rheumatoid Arthritis-Associated Interstitial Lung Disease Subtypes Identified
核心概念
Older age, male sex, and seropositivity are associated with a higher risk for the usual interstitial pneumonia (UIP) subtype of rheumatoid arthritis-associated interstitial lung disease (RA-ILD), while only seropositivity is linked to the nonspecific interstitial pneumonia (NSIP) subtype.
摘要
The study examined the risk factors associated with different subtypes of rheumatoid arthritis-associated interstitial lung disease (RA-ILD) using data from two cohorts in the Mass General Brigham Healthcare system.
The researchers identified 208 patients with RA-ILD and 547 control participants with rheumatoid arthritis (RA) but no ILD. RA-ILD subtypes were determined using high-resolution computed tomography (HRCT) imaging.
The key findings are:
- The RA-UIP subtype, which has the worst prognosis, was associated with older age at RA diagnosis, male sex, and seropositivity.
- The RA-NSIP subtype was significantly associated only with seropositivity.
- Nonfibrotic ILDs were significantly associated with positive smoking status and seropositivity.
- The combination of male sex, seropositivity, and positive smoking status was associated with a nearly sevenfold increased risk for RA-UIP.
The authors suggest that RA-ILD subtypes may have distinct risk factor profiles, emphasizing the importance of understanding RA-ILD disease heterogeneity to inform screening and prognostication strategies.
自定义摘要
使用 AI 改写
生成参考文献
翻译原文
翻译成其他语言
生成思维导图
从原文生成
访问来源
www.medscape.com
RA Lung Disease Subtypes Have Distinct Risk Factor Profiles
统计
Older age at RA diagnosis was associated with a higher risk for RA-UIP (OR 1.03 per year, 95% CI 1.01-1.05).
Male sex was associated with a higher risk for RA-UIP (OR 2.15, 95% CI 1.33-3.48).
Seropositivity was associated with a higher risk for RA-UIP (OR 2.08, 95% CI 1.24-3.48) and RA-NSIP (OR 3.21, 95% CI 1.36-7.56).
Positive smoking status was associated with a higher risk for nonfibrotic ILDs (OR 2.81, 95% CI 1.52-5.21).
The combination of male sex, seropositivity, and positive smoking status was associated with a nearly sevenfold increased risk for RA-UIP (OR 6.89, 95% CI 2.41-19.69).
引用
"These findings suggest that RA-ILD subtypes may have distinct risk factor profiles and emphasize the importance of further efforts to understand RA-ILD disease heterogeneity to inform screening and prognostication strategies."
从中提取的关键见解
by Edited Javed... 在 www.medscape.com 09-26-2024
https://www.medscape.com/viewarticle/rheumatoid-arthritis-lung-disease-subtypes-have-distinct-2024a1000hhy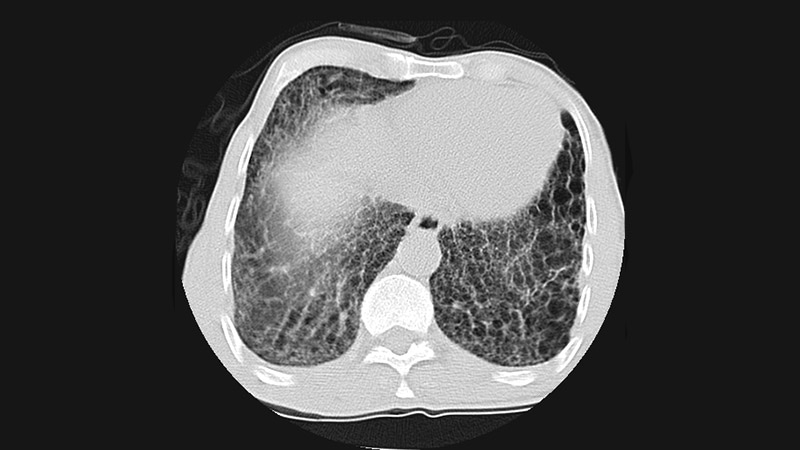
更深入的查询
What are the potential underlying mechanisms that explain the different risk factor profiles for RA-ILD subtypes?
The distinct risk factor profiles for rheumatoid arthritis–interstitial lung disease (RA-ILD) subtypes, particularly RA-UIP and RA-NSIP, may be attributed to several underlying mechanisms. Firstly, the association of older age and male sex with RA-UIP suggests that hormonal and age-related biological changes could influence lung pathology. For instance, androgens may modulate immune responses and fibrosis, potentially leading to a more severe lung disease phenotype in males. Additionally, older age is often linked to cumulative exposure to environmental factors, such as smoking, which is a known risk factor for lung fibrosis.
Seropositivity, particularly for rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPAs), is a common risk factor across both subtypes. These autoantibodies may contribute to lung inflammation and fibrosis through immune-mediated mechanisms, promoting the recruitment of inflammatory cells and the deposition of extracellular matrix components in the lung tissue. The differing associations of seropositivity with RA-UIP and RA-NSIP may reflect variations in the underlying immunopathological processes, where RA-UIP is characterized by more pronounced fibrotic changes compared to the inflammatory nature of RA-NSIP.
Furthermore, the presence of nonfibrotic ILDs being significantly associated with positive smoking status indicates that environmental exposures can interact with genetic predispositions, leading to different disease manifestations. The interplay between genetic susceptibility, environmental triggers, and immune dysregulation likely contributes to the heterogeneity observed in RA-ILD subtypes.
How can the findings of this study be used to develop targeted screening and management strategies for patients with RA-ILD?
The findings from this study highlight the importance of identifying distinct risk factors associated with different RA-ILD subtypes, which can inform targeted screening and management strategies. For instance, recognizing that older age, male sex, and seropositivity are significant risk factors for RA-UIP can lead to more proactive screening protocols for these high-risk groups. Clinicians may consider implementing regular high-resolution computed tomography (HRCT) scans for early detection of lung disease in patients with these characteristics.
Moreover, the identification of seropositivity as a common risk factor for both RA-UIP and RA-NSIP suggests that monitoring serological markers could be a valuable tool in assessing the risk of developing ILD. This could facilitate timely interventions, such as the initiation of disease-modifying antirheumatic drugs (DMARDs) or corticosteroids, to manage inflammation and potentially slow disease progression.
In terms of management, understanding the distinct profiles of RA-ILD subtypes can guide personalized treatment approaches. For example, patients with RA-UIP may benefit from antifibrotic therapies, while those with RA-NSIP may require more aggressive immunosuppressive strategies. Additionally, lifestyle modifications, such as smoking cessation programs, could be emphasized for patients identified as having nonfibrotic ILDs, given the strong association with smoking status.
What other clinical or biological factors, beyond those examined in this study, may contribute to the development and progression of different RA-ILD subtypes?
Beyond the demographic and serological factors examined in this study, several other clinical and biological factors may contribute to the development and progression of different RA-ILD subtypes. Genetic predisposition plays a crucial role; specific genetic polymorphisms associated with RA and lung disease may influence individual susceptibility to ILD. For instance, variations in genes related to immune regulation and fibrosis could affect the severity and type of lung involvement.
Comorbidities, such as obesity, diabetes, and cardiovascular disease, may also impact the progression of RA-ILD. These conditions can exacerbate inflammation and alter immune responses, potentially leading to worse outcomes in patients with RA-ILD. Additionally, the presence of pulmonary hypertension or other respiratory conditions may complicate the clinical picture and influence management strategies.
Biomarkers of inflammation and fibrosis, such as serum levels of cytokines (e.g., IL-6, TNF-alpha) and matrix metalloproteinases, could provide insights into disease activity and progression. The role of the microbiome in modulating immune responses and inflammation is an emerging area of research that may also contribute to the heterogeneity of RA-ILD subtypes.
Finally, environmental exposures beyond smoking, such as occupational dust, air pollution, and viral infections, may play a significant role in the pathogenesis of RA-ILD. Understanding these multifactorial influences is essential for developing comprehensive management strategies and improving patient outcomes.
0